Originally published on June 23, 2010
C.L. asks, “What are the chances of esophageal or tracheal rupture, or subcutaneous emphysema with reinsertion of a dislodged tracheostomy tube?”
Answer: I have never encountered esophageal nor tracheal rupture during reinsertion of a dislodged tube. Nor am I aware of any reports in the literature. Theoretically, it could occur if the tube was placed with great force and without an obturator to cushion the tip, or perhaps in combination with friable tissue. However, ruptured esophagus and ruptured trachea have been reported as a complication during the tracheotomy procedure, particularly with the percutaneous technique.
As for subcutaneous emphysema, this can occur if the tube is inserted into a false passage and positive pressure is applied, forcing air into the subcutaneous tissue. During the early postoperative period, tube security should be a priority. When replacing a tube into a mature stoma, and prior to application of positive pressure, it is important to confirm placement by passage of a suction catheter with return of tracheal secretions.
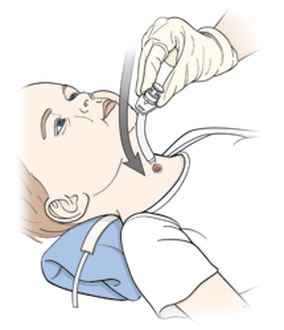
When replacing a tube, technique is also important. An initial 90 degree approach, followed by a caudal turn is the recommended technique. A premature caudal turn can result in placement into a false passage.